News
-
17 February 2014
"Vita" hospital performs innovative surgic... -
13 May 2013
FREE ORTHOPAEDIC EXAMINATIONS AT ‘VITA’ -
03 September 2012
Injuries from motorcycle accidents fill th... -
11 May 2012
Surgeons from "Vita" operated successfully... -
11 March 2009
Specialized NUCLEAR MAGNET RESONANCE for d...
 Surgery performed in "VITA" Hospital
Surgery performed in "VITA" Hospital|
Hip Arthroscopy 16.08.2012 Dr. Chanko Chankov
|
|
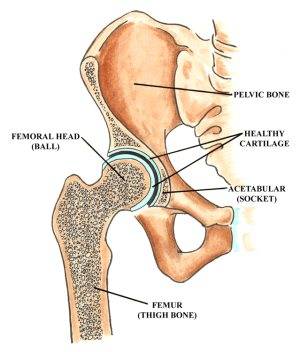
The hip joint is a “ball and socket” joint located where the thigh bone (femur) meets the pelvic bone. The upper segment (“head”) of the femur is a round ball that fits inside the cavity in the pelvic bone that forms the socket, also known as the acetabulum. The ball is normally held in the socket by very powerful ligaments that form a complete sleeve around the joint capsule. Both the ball and socket are covered with a layer of smooth cartilage, each about 1/8 inches thick. The cartilage acts as a sponge to cushion the joint, allowing the bones to slide against each other with very little friction. Additionally, the depth of the acetabulum (socket) is increased by a fibrocartilaginous rim called a labrum that lines the rim of the socket and grips the head of the femur, securing it in the joint. The labrum acts as an “o-ring” or a gasket to ensure the ball fits into the socket.
The hip joint is the largest ball and socket joint in the body and goes through seven million movement cycles per year in the average person. The hip joint can be prone to wear and tear and arthritis in older individuals. However, younger people can also develop a variety of hip joint problems that can affect walking, running, sport and daily activities.
What is a hip arthroscopy? To say hip arthroscopy is a difficult technique would be something of an understatement. It is much more technically challenging than the more common knee arthroscopy and the learning curve for a surgeon new to hip arthroscopy is extremely steep. The gap between the ball and socket of the hip joint is very small; as recently as 1931, doctors thought that it was impossible to place a needle here. Today it has become possible to view the inside of the hip joint using a keyhole technique and a tiny endoscopy camera. Tiny surgical instruments can also be introduced to carry out treatments. Hip arthroscopy, or a “hip scope,” is a minimally-invasive procedure. The use of an arthroscope means that the procedure is done using 2-3 small incisions (approximately 1/4-1/2 inch long) rather than a more invasive “open” surgery that would require a much larger incision. These small incisions, or “portals", are used to insert the surgical instruments into the joint.
Aiding other advances in arthroscope technology, the flow of saline through the joint during the procedure provides the surgeon with excellent visualization. The surgeon is also aided by fluoroscopy, a portable x-ray apparatus that is used during the surgery to ensure that the instruments and arthroscope are inserted properly. Hip arthroscopy usually takes between 45 minutes and 2 hours, depending on the complexity of the operation.
The procedure is normally done as an “outpatient” surgery, which means the patient has the surgery in the morning and can go home that same day. Normally, the patient is under regional anesthesia. Under regional anesthesia, the patient is numbed only from the waist down and does not require a breathing tube. Sometimes under special conditions it can be done under general anaesthetic. Traditional open surgery of the hip joint is a major procedure and involves large cuts through the skin and the muscles to get to the joint. Arthroscopy of the hip, however, allows the joint to be visualized with tiny telescopes and cameras and for pathology within the joint to be treated with specialized probes, through tiny skin incisions with minimal damage to the tissues.
What can be treated by hip arthroscopy? Hip arthroscopy can be used to treat several conditions that can result from sports injuries, avoiding the need for more extensive hip surgery:
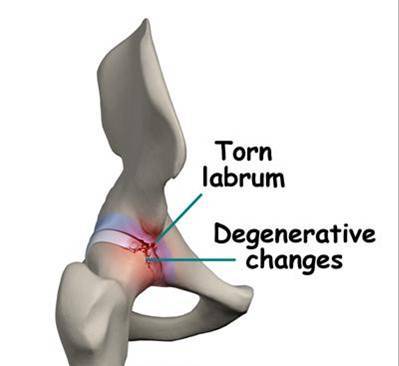
How do I know if I need this surgery? Usually, this surgery is indicated in people who have pain that can be localized to the hip, but with minimal findings on x-ray. As such, many of these problems can be hard to define, and patients occasionally go months to years without a specific diagnosis, especially if the physician does not have a lot of experience with these diseases. Some diagnoses (synovial chondromatosis, polyvillonodular synovitis) can be made using special studies like CT scans or MRIs. Other problems, such as tears of the acetabular labrum, might not show up on any of the tests and can only be diagnosed with physical examination, listening to the patient history, and exclusion of other diseases.
Possible complications Hip arthroscopy is a very safe procedure. The most common side effects are discomfort around the hip area and slight bruising. Numbness around the foot or groin is seen in about 5% of cases. Serious complications such as infection, bone fracture or permanent nerve injury are extremely rare. Recovery Process Generally, most patients have the surgery performed on a same day basis - no overnight stay in the hospital is required. Often patients are able to tell that night or the next day that their hip feels better. This is usually followed by a recurrence of the pain, which lasts a few weeks, then gradual resolution of the pain. This recurrence is usually from bleeding into the joint after surgery causing irritation of the joint lining.
Following the procedure, patients are normally given crutches to use for several days to minimize weight-bearing. A post-operative appointment is normally held a week after the surgery to remove sutures. Following this appointment, the patient normally begins a physical therapy regimen that improves strength and flexibility in the hip. After six weeks of physical therapy, many patients can resume normal activities, but it may take 3-6 months for one to experience no soreness or pain following physical activity. As no two patients are the same, regular post-operative appointments with one’s surgeon is necessary to formulate the best possible recovery plan. Most patients are able to drive a car the following day. People with desk jobs may return to work as early as 1-2 weeks after the arthroscopy, while people in heavy manual employment may require 6 weeks off work. Sport can often be reintroduced from 4-6 weeks. 80% of high level and elite athletes return to match fitness by 16 weeks. A small number of patients may have ongoing mild discomfort for up to 3-4 months after the procedure, depending on the degree of joint damage present at arthroscopy. Benefits of hip arthroscopy Studies have shown that 85-90% of hip arthroscopy patients return to sports and other physical activities at the level they were at before their onset of hip pain and impingement. The majority of patients clearly get better, but it is not yet clear to what extent the procedure stops the course of arthritis. Patients who have underlying skeletal deformities or degenerative conditions may not experience as much relief from the procedure as would a patient with simple impingement. The benefit of hip arthroscopy is that the recovery is much simpler than for open hip surgery. Patients can typically put as much weight as tolerated on the hip immediately following surgery (check with your doctor as some procedures may limit weight bearing). Hip arthroscopy is indicated when conservative measures fail to relieve symptoms related to femoro-acetabular impingement, a condition that has been poorly understood and under-treated in the past. Advances have made hip arthroscopy a safe and effective alternative to open surgery of the hip, a tremendous advantage in treating early hip conditions that ultimately can advance to end-stage arthritis. |